Introduction
The microbiome (microflora or microbiota) consists of trillions of microorganisms (bacteria, fungi, protozoa, viruses) that colonize the skin, nose, digestive system, lungs, and vagina but the most substantial quantity is in the colon and small intestine.
Even the microbiome is known as a "supporting organ," since it plays critical roles in maintaining our body's physiological functions.
At the intestinal stage, the microbiome contains at least 1,000 different bacterial species with more than 3 million genes (150 times more than human genes) and weighing up to 2 kg.
One-third of the gut microbiome is common to most people, while two-thirds are unique to each of us. In other words, it's like an individual identity card, just like the fingerprint, which is unique.
Until birth, babies are practically sterile, having only their body cells. But in the first few years of life, the growing child takes microbes from various sources:
- Initially, the first microbes are inherited from the mother through natural birth and breastfeeding.
The amount and type of bacteria inherited, depend only on the species that exist in the mother.
These early bacteria, with which the baby is colonized, seem to help him fight against allergies, asthma, inflammatory bowel disease, obesity, and diabetes.
Several studies have linked conception by Caesarean region with possible infections of the later adult, and lack of breastfeeding. It is therefore advised that the baby be breastfed wherever possible and as long as possible.
2. Subsequently, through exposure to microbes in the atmosphere (playgrounds, dust, pets, clothes, stress, and pollution) and by diet, which can change the human microbiome either in a way that is beneficial to health or in a risk factor for different conditions.
The "obsession of cleanliness," i.e., the exaggerated concern for the sterilization and disinfection of all objects with which a child or an adult comes into contact, may have a negative impact on health in the short and long term.
Factors that imbalance the intestinal microbiome
Diet is the element that has a permanent nature of disruption or rebalancing.
The microbiome is made up of microorganisms that can be both beneficial and potentially harmful.
In a healthy body, the two groups coexist without any problems.
Nevertheless, when this equilibrium is disrupted – caused by infectious diseases, other foods, medications, surgery or excessive use of antibiotics – intestinal dysbiosis (which has the following symptoms: stomach problems, diarrhea, vomiting, halitosis, bloating and rash) and the sensitivity of the body to diseases.
A diet rich in processed sugars and, in particular, low in dietary fiber, consumption of carbonated drinks, burgers, fast food, high-fat trans foods (pastry, cookies, muffins)-all of which have a detrimental effect on the human intestinal population.
On the other side, an antibiotic warning signal should be activated. We harm some of the microorganisms in the stomach, oral and vaginal cavities, contributing to the increased production of others.
Therefore, infections such as candidiasis or diarrhea triggered by Clostridium difficile occur.
In order to prevent or treat these infections, it is recommended that substances with probiotic and prebiotic effects should be administered by diet or dietary supplements during antibiotic treatment and at least two weeks after that.
Introduction
Genetic sequencing has wholly changed our comprehension of the tree of life and the position of humans inside it.
The introduction of the DNA sequencing method of Sanger in 1977 and the DNA amplification process of polymerase chain reaction (PCR) in 1983 led to a rise of genetic data that assessed the phylogeny of humans and the great apes, dismissed the biological definition of race in humans, and reconstructed the world's civilizations.
The diverse microbial species that inhabit the human body, denominated as the human microbiome, constitute a large amount of genetic and functional diversity that far exceeds that of our own nuclear and mitochondrial genomes).
Increased recognition of the role of microbiomes in the functions of basic host life, disease etiology, and even speciation, disputes traditional views on the definition of biological species and raises the question as to whether or not ancient human microbiomes would also be examined to address broader issues in human evolution.
This study will address the symbiosis and their microbiomes and will examine new developments in ancient microbiome research in the field of research. They suggest that we can only truly appreciate what it means to be human by studying our microbiomes today and in the past, too.

The Gut Microbiota
Additional Information
There is a whole new scientific vocabulary and an explosion of GUT knowledge that increases each year steadily.
Stomach symptoms have increased over the past two decades, and many people are diagnosed with diarrhea, constipation, vomiting, coeliac disease, malabsorption of fructose, leaky gut, intestinal permeability, Crohn's disease, ulcerative colitis, SIBO (overgrowth of small intestinal bacteria), malabsorption of fat, indigestion, and cancer of the alimentary canal.
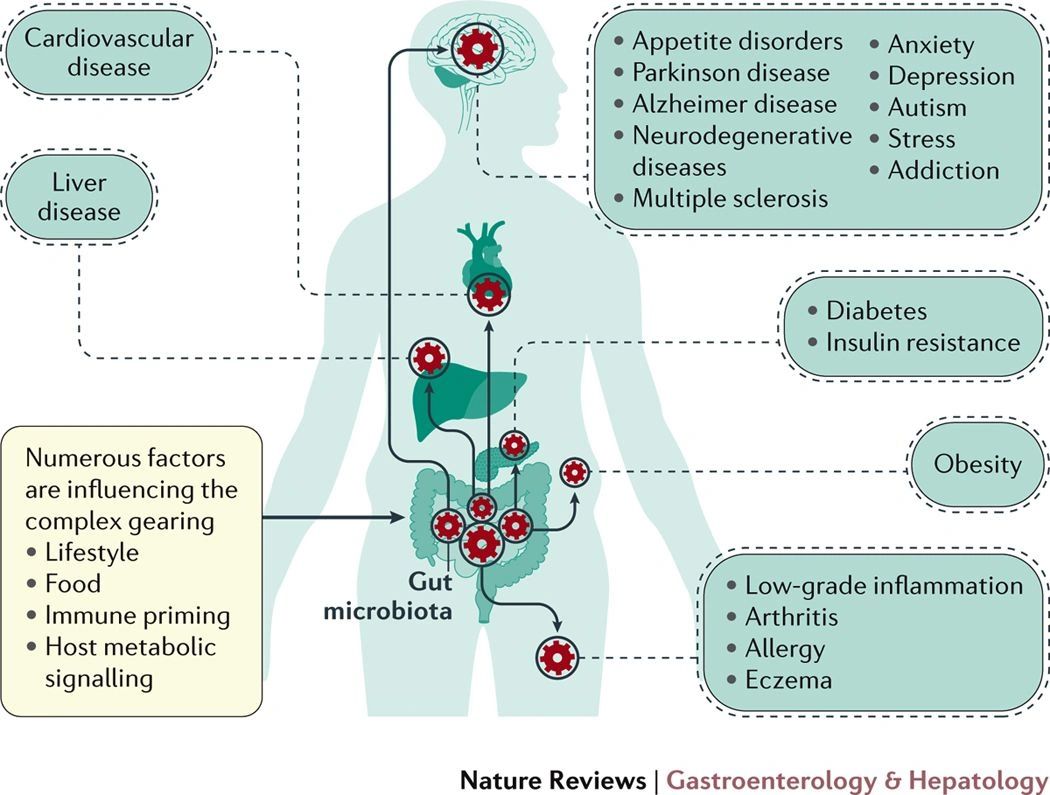
Systemic diseases involving heart disease, diabetes, cancer, and autoimmunity have also undergone a steady rise.
Autoimmunity is a broad term comprising, most prominently, one hundred plus disorders, multiple sclerosis, type 1 diabetes, lupus, hashimotos, sepulchers, add-ons, Parkinson's and rheumatoid arthritis.
Previously, a majority of people reported to their physicians, identified their symptoms, diagnosed illness, and prescribed medication and confirmed that their wellbeing or symptoms had nothing to do with their diet.
The food we bring into the body affects every cell and its entire biochemistry, thus affecting every system and every organ.
Not only do we acknowledge that the food we eat will give us the strength and foundation of the body, but now we realize that any food we eat will influence our DNA.
The GUT has a population of bacteria, viruses, fungi, mushrooms, and yeasts. Those kinds of microbes live symbiotically with us, help us digest, prevent infection, make vitamins, amino acids, fats, etc.
The health of our Microbiota is essential to wellbeing. Such bugs live symbiotically with us, helping us digest, combat diseases, produce vitamins, amino acids, fats, etc.
Our modern lifestyle, food contaminated with pesticides, pollutants in nature and our homes, heavy antibiotic use, food consumption, refined, packaged foods, inadequate sleep and hygiene, insufficient sunlight, all contribute to dysbiosis (sickness). We get sick when there's dysbiosis in the GUT and Microbiota.
While most of us have become aware of probiotics due to physician and pharmacist recommendations, prebiotics are less well known.
There are significant differences between the two, and there are also different health benefits to the human body.
Although probiotics have proved effective in handling some gastrointestinal issues, they do not have the same power as prebiotics.
Therefore, probiotics identify living microorganisms that colonize our digestive tract (mostly bacteria). Such microorganisms help us digest food, a cycle in which food consumes nutrients and vitamins, creates vitamins B and K, and prevents the production of other microorganisms that could damage our health.
Probiotics are found both in the form of dietary supplements, which we can purchase from pharmacies, but are also present in certain types of fermented foods for which: sour cabbage, pickles yogurt, kefir, soft fermented cheeses bread dough.
To enjoy the benefits of probiotics obtained from food sources, these bacteria have to be alive and healthy throughout the food's shelf life to survive digestion and ultimately colonize the gut. Therefore, by regulating the harmful bacteria, they help maintain the health of the digestive system.
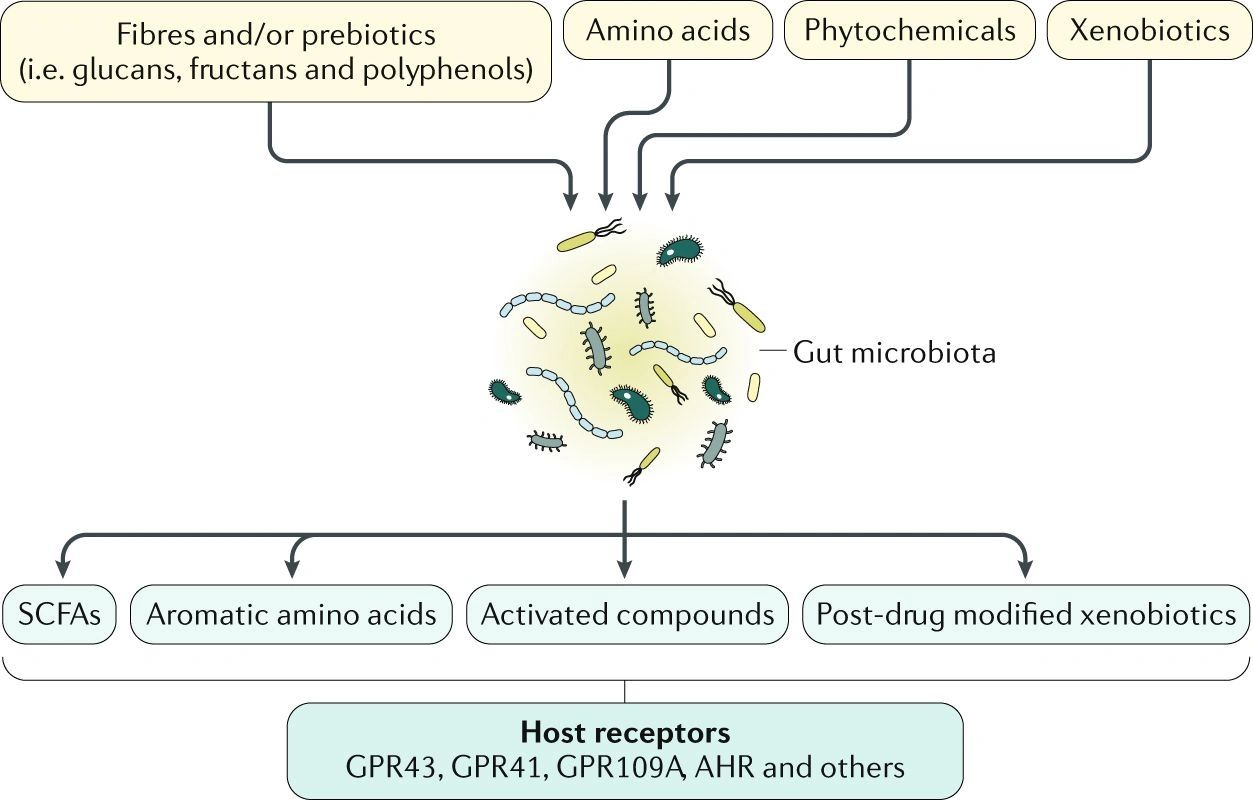
On the other hand, to help maintain them, prebiotics are often described as probiotics for "food." Prebiotics are soluble fibers and other groups of carbohydrates, such as starch and sugars called oligosaccharides that are fermented by bacteria.
Prebiotic sources include asparagus leeks from bananas potatoes, onions, garlic chicory, flakes from artichoke oatmeals.
Prebiotics have many benefits in helping to better digest minerals such as calcium and magnesium, shielding the body from bacterial infections, combating bowel pain, diarrhea, and irritable bowel syndrome.
So we have to be careful to add a variety of vegetables and as many fibers into our diet to maintain the health of the digestive tract that determines the health of the entire body.
What are prebiotics?
Prebiotics are non-digestible carbohydrate compounds. Specifically, they are a type of fiber, best known as oligosaccharides. As a mildly amusing detail, all prebiotics are fibers, but not all fibers are prebiotics.
The non-digestible components of foods are prebiotic fibers.These are known to travel undigested through the small intestine before they enter the colon, where the intestinal microflora (bacteria) ferment them. We promote the growth and development of bacteria in the digestive system when fermented, which can provide potential health benefits.
Prebiotics are different from probiotics.
In short, probiotics in the digestive tract are good bacteria. These support the process of digestion and have other potential health benefits. They are quite frequently found in fermented foods like pickled cabbage and kefir. Prebiotics aren't crops that exist. These are fibers that are non-digestible and nourish probiotic bacteria.
Why should we consume prebiotics?
There are many good reasons why prebiotics should become a daily part of your diet. Research has shown that higher prebiotic intake can offer the following health benefits:
- Healthier gut because beneficial bacteria prevent harmful bacteria from entering the gastrointestinal tract
- Ensure proper functioning of the immune system
- Weight loss risk by controlling appetite
- Reduction of inflammation associated with inflammatory bowel disease
- Reducing the risk of cardiovascular disease by regulating cholesterol levels
- Reduce the risk of type 2 diabetes by improving the rate of glucose uptake
- Improvement and strengthening of the digestive system
- Increased availability of minerals in the body
- Decreased risk of colon cancer
For the most part, fiber ingested by the diet is the primary source of prebiotics-specifically certain types of fruits, vegetables, and carbohydrates. Inulin, which is a soluble dietary fiber, comes from raw garlic, asparagus, and onions.
If you're worried you don't have enough prebiotics in your diet, supplements in a concentrated form may provide the required protection. You can also make sure of your daily intake of prebiotics and some food.
For the most part, fiber ingested by the diet is the primary source of prebiotics-specifically certain types of fruits, vegetables, and carbohydrates. Inulin, which is a soluble dietary fiber, comes from raw garlic, asparagus, and onions.
Indeed, it has been demonstrated that inulin is prebiotic. The difference between certain difficult-to-digest fibers is that inulin is a water-soluble fiber. Also, it is found in onions, leeks, garlic, asparagus, artichokes, and many other foods.
If you don't think you consume enough prebiotics in your diet, inulin is an easy-to-mix prebiotic powder supplement. Just add 1-2 cups of 5 g of water in a shake or smoothie once a day.
The best food sources of prebiotics
Vegetables are the best sources of prebiotics, but because the fibers break down through cooking, it's good to eat them raw to get the best effect. Other healthy prebiotic sources are whole grains, green bananas, or potatoes.
More prebiotics can be consumed in the diet through isolated carbohydrates (known as galactooligosaccharides and transgalactooligosaccharides).
The following foods are worth considering for an increase in the intake of prebiotics:
Legumes (such as beans, lentils, and peas)
- Whole wheat
- Oats
- Honey
- Boiled and chilled potatoes
- Root of raw chicory
- Inulin
- Raw garlic
- Raw term
- Raw or cooked onions
- Raw asparagus or cooked al dente
- Acacia gum
- Green bananas
- Whole psyllium shells
Conclusion
Prebiotics are non-digestible sources of fiber, and inulin is a water-soluble variety.
Prebiotics are needed to develop healthy (beneficial) bacteria that support both the digestive system and other functions, such as the immune system.
Prebiotics may be obtained from dietary sources, mainly fruit and vegetables, but prebiotic supplements are available to ensure that the uptake meets the daily requirement.